The Chronic Miasms - Part Three & Four
By Dr. Will Taylor
Introduction by Editors:
Dr. Will Taylor has written a six-part essay on the Chronic Miasms — a detailed exploration of the development and evolution of homeopathic miasmatic theory, tracing how Samuel Hahnemann first arrived at these ideas and how they have subsequently been understood, interpreted, and expanded within the profession. The series offers an in-depth study of Hahnemann’s thinking, examining questions such as whether miasms are solely acquired infectious influences or also inherited predispositions, whether there may be more than three miasms, and how such an expansion might be rationalized within homeopathic philosophy and practice.
The essays also investigate Hahnemann’s understanding of the roots of chronic disease and the practical implications this carries for prescribing in long-standing chronic conditions. Through careful historical and philosophical analysis, Dr. Taylor illuminates both the continuity and evolution of miasmatic thought across generations of homeopaths.
We have been publishing this important series in installments. Parts One and Two appeared in Volume 20, Issue 1. Parts Three and Four are published in the present issue, with Five and Six scheduled for the Winter Solstice Issue.
Part Three
Relevance of the chronic miasms to the practice of homeopathy
To the 3rd American edition of the Organon, Hering wrote:
“What important influence can it exert, whether Homoeopathy adopts the theoretical opinions of Hahnemann or not, so long as he holds fast the practical rules of the master, and the Materia Medica of our school? What influence can it have, whether a physician adopts or rejects the Psora theory, so long as he always selects the most similar remedy possible?”
We might ask, despite how fascinating it might be to speculate on or observe the origins of chronic disease, how this might inform our practice of healing? Does Hahnemann’s focus on the nature of chronic disease conflict with that audacious footnote to aphorism 1 in the Organon?
His mission is not, however, to construct so-called systems, by interweaving empty speculations and hypotheses concerning the internal essential nature of the vital processes and the mode in which diseases originate in the invisible interior of the organism, (whereon so many physicians have hitherto ambitiously wasted their talents and their time) ; nor is it to attempt to give countless explanations regarding the phenomena in diseases and their proximate cause (which must ever remain concealed), wrapped in unintelligible words and an inflated abstract mode of expression, which should sound very learned in order to astonish the ignorant—whilst sick humanity sighs in vain for aid. Of such learned reveries (to which the name of THEORETIC MEDICINE is given, and for which special professorships are instituted) we have had quite enough, and it is now high time that all who call themselves physicians should at length cease to deceive suffering mankind with mere talk, and BEGIN now, instead, for once to ACT, that is, really TO help and to cure.
Hahnemann observed that although homœopathy had proved itself successful in the treatment of acute individual, sporadic, epidemic, and venereal diseases, its success in chronic disease was less than he might hope for. His explanation was that chronic disease invariably expresses itself incompletely (“defectively,” in Pierre Schmidt’s terminology), and required “completion” as he’d described for epidemic disease (Organon, §s101-104), “one-sided” and “local” disease (§s172-193), so-called “one-sided” “somatic” and “mental/emotional” disease (§s210-220), and intermittent & alternating disease §s231-235). In order to do this, one needed an appreciation of the disease in its entirety, beyond its “defective” presentation in an individual.
The problem with neglecting chronic disease “theory” and merely selecting the most similar remedy possible in the treatment of chronic disease, is that we’ll often find ourselves working with an incomplete, “defective” case. We may have enough of a totality to get by, but can improve our odds considerably with attention to the “completed” disease as a whole.
In the case of Syphilis, this description was readily at hand, in the many cases of both acute and chronic syphilis encountered in practice. Between the 18th and 19th century, syphilis affected nearly 20% of the urban population in Europe (1). Hahnemann carefully assembled a picture of primary, secondary, latent, and tertiary syphilis in The Chronic Diseases.
Sycosis was of principal interest as potentially confusable with the condylomata secondary syphilis, and was responsible for only a minor percentage of chronic disease in Hahnemann’s experience; his description of its chronic expressions was limited to “contraction of the tendons of the flexor muscles, especially of the fingers.”
The estimated 7/8ths of chronic diseases not attributable to venereal origin presented a challenge that occupied Hahnemann for many years. In 1821, Hahnemann moved from Leipzig, a center of European intellectual culture, to the relatively backwater town of Köthen, under the protection of Prince Ferdinand. His primary duties were to attend to the prince’s health, which required little attention, a slow practice of locals, and cases taken by correspondence. He had much time on his hands to attend to development of the Materia Medica Pura and to focus on scrutinizing those cases of chronic disease that could not be attributed to venereal disease, medical disease (§74), or external sustaining factors (§77). He concluded that this vast diversity of chronic disease could be attributed to a single chronic miasm (infectious/contagious disease) which he termed Psora, from the Greek word for an itching skin eruption, the principal presenting symptom in the primary, acute phase of disease. The implication for our practice is not so much identification of or attribution to a specific infectious agent, which unlike Syphilis and Sycosis remains mysterious, but our ability to “complete” our case of non-venereal chronic disease with the description he developed. In volume 2 of The Chronic Diseases, Hahnemann presented the pure materia medica of 48 remedies he determined to address the common expressions of Psora, his “antipsoric” remedies, led by Sulphur, which he considered a near-specific. Boenninghausen later assembled these, with their common and differentiating expressions, in his Systemic Alphabetic Repertory of Antipsoric Remedies.
By selecting remedies that bear similitude to the visible aspects of a chronic psoric case that are also known to be “antipsorics,” we increase the likelihood that our “kinda-sorta-closicums” will bear similitude to the partially revealed / partially unrevealed totality of the “defectively” presenting case.
A practice proposed by some is to “clear” chronic miasms, as if these were merely phenomena somehow extraneous to disease impeding response in healing, with a specific remedy (often the proposed nosode or a genus remedy such as Sulphur for Psora) in order to permit a simillimum to act. We see this formalized in Francisco Eizayaga’s “Layers” approach, in which the chronic miasms are envisioned as “morbid terrain” lying between the “prodromal” General disease and a fundamental “constitution,” to be addressed after the General disease is treated and before attention to a “constitutional” prescription. Such “layers” do not really exist in our patients, but may appear dynamically as successive challenges, much as successive challenges that appear consequent to the strokes we play in working our way through a game of golf.
The remedy for a chronic miasm is not intended to “clear” an obstacle, but to treat the chronic (miasmatic) disease of the person. This will often require a succession of remedies, not to address existing “layers,” but as outlined in Hahnemann’s directions for working with too few remedies (§162-171) and with “one-sided” disease (§s 177-184).
The prescription of the chronic miasmatic nosode or a generic anti-miasmatic remedy will not “clear the miasm,” but, if it acts at all, will act as the “imperfectly homeopathic remedy” described in §162-171 and 177-184 in the Organon; If a similimum is a similar remedy and a simillimum (2 Ls) the most similar, I describe these as “kinda-sorta-closicums.” If sufficiently similar, it will act partially, but give rise to new “accessory symptoms” which belong in part to this remedy, but “are, however, at the same time, symptoms of the disease itself, although they may hitherto never or very rarely perceived; some symptoms which the patient had never previously experienced appear, or others he had only felt indistinctly become more pronounced” (§180). These, now added to the remaining totality, provide a more complete image of the disease. “In like manner, after each new dose of medicine has exhausted its action, when it is no longer suitable and helpful, the state of the disease that still remains is to be noted anew with respect to its remaining symptoms, and another homeopathic remedy sought for, as suitable as possible for the group of symptoms now observed, and so on until the recovery is complete” (§184). This process may task our prescribing and case management skills, as well as the fortitude of the patient in weathering a potential cascade of new symptoms in the course of cure.
This is not necessarily territory for the faint-hearted; once we embark on it, we’re committed to following it through, like playing our way through a golf course , potential sand traps, water hazards, roughs, and all (I don’t play golf, but the metaphor is compelling). We want each successive kinda-sorta-closicum to be as close to a simillimum as we can make it, in order to act at all, and to land us on the green rather than in the rough, rather than merely pull a standard prescription out of our back pocket. The initial prescription may appear to smack of routinism, but followup is anything but. Kent’s 1888 Lecture on the Second Prescription, which needs some modification for the split dose posology Hahnemann introduced after c. 1828, details this process well.
Hahnemann may have opened many of his psoric cases in his Paris years with Sulphur in this manner, but last I looked, neither I nor you are Samuel Hahnemann. Here posology, as well as accuracy in remedy selection, comes into play; Hahnemann modified his posology as he began to focus on the treatment of chronic disease, adopting the “split dose” of centesimals in water (described in the 1837 preface to the 3rd edition of The Chronic Diseases) & eventually his “medicaments au globule” (LMs; described in the 1843 6th edition of the Organon), given in divided dose in water; in my golf metaphor, substituting a series of putts for drives. In homeopathy, unlike golf, we don’t keep score & only tally the ball in the hole.
Constantine Hering, preface to the American translation of the 3rd edition of Hahnemann’s The Chronic Miasmshttps://courses.homstudies.com/mod/page/view.php?id=620
Samuel Hahnemann, Organon of the Art of Healing, 6th edition
Pierre Schmidt, 1980, Defective Illnesses https://courses.homstudies.com/mod/page/view.php?id=500
James Tyler Kent, 1888, Lecture on the Second Prescriptionhttps://courses.homstudies.com/mod/page/view.php?id=475
Will Taylor, 2025, Homeopathic Posologyhttps://payhip.com/b/wmRyo
Part Four
The chronic miasms and acute disease
The chronic miasms are chronic diseases - diseases “of such a character that, with small, often imperceptible beginnings, dynamically derange the living organism, each in its own peculiar manner, and cause it gradually to deviate from the healthy condition, in such a way that the automatic life energy, called vital force, whose office is to preserve the health, only opposes to them at the commencement and during their progress imperfect, unsuitable, useless resistance, but is unable of itself to extinguish them, but must helplessly suffer (them to spread and) itself to be ever more and more abnormally deranged, until at length the organism is destroyed” (Organon, §72), contrasting these with acute diseases “which have a tendency to finish their course more or less quickly, but always in a moderate time.”
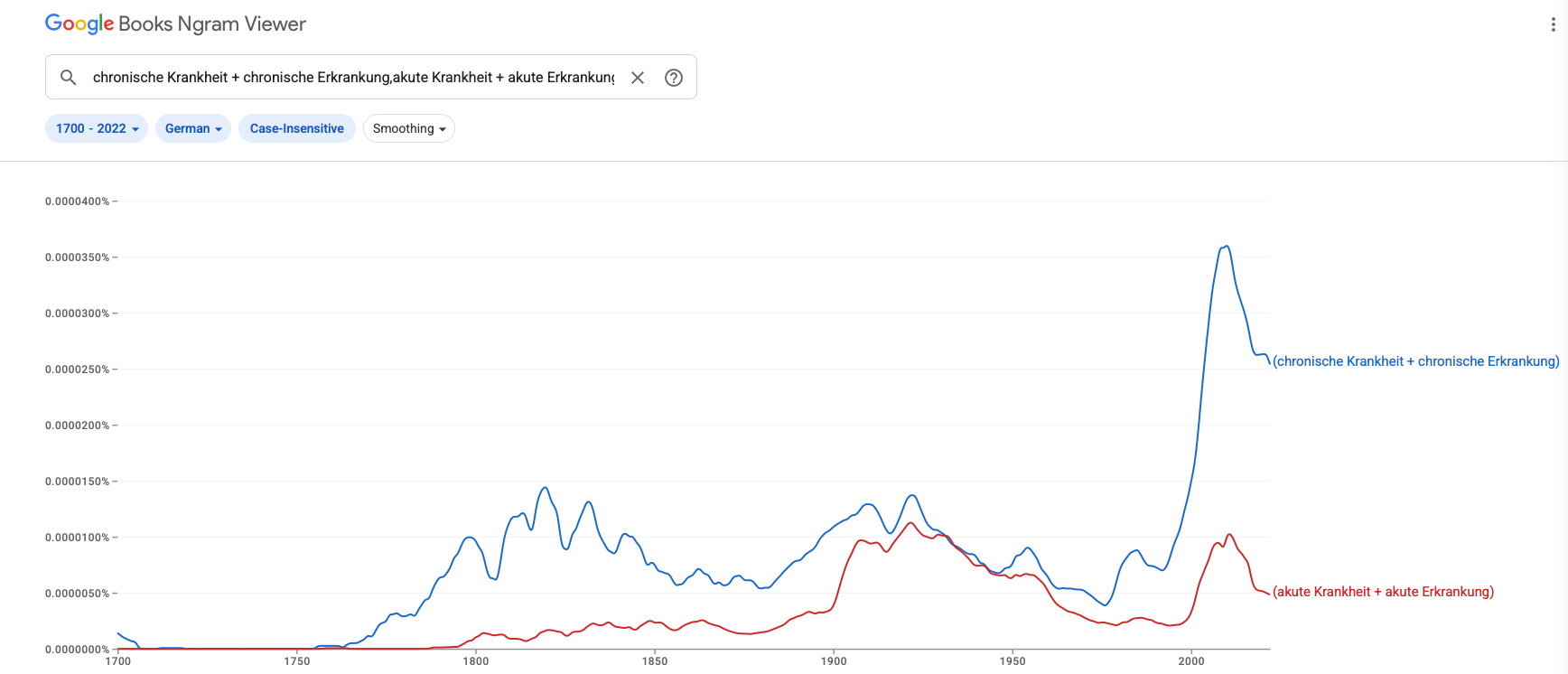
Fig. 1 - appearance of chronische Krankheit + chronische Erkrankung, (chronic disease), akute Krankheit + akute Erkrankung (acute disease) in the German literature, 1700-present
James Tyler Kent asserted that Psora (which, recall, he equated with original sin):
“is the beginning of all physical sickness … Had Psora never been established as a miasm upon the human race, the other two chronic diseases would have been impossible, and susceptibility to acute diseases would have been impossible. All the diseases of man are built upon Psora ; hence it is the foundation of sickness ; all other sickness came afterwards. Psora is the underlying cause, and is the primitive or primary disorder of the human race.” (Kent, Lectures on Homeopathic Philosophy, Lecture 18)
Hahnemann did suggest that many individual acute diseases (§73) “are generally only a transient explosion of latent Psora,” acutes predicated on chronic disease, but did not ascribe all individual acutes, or sporadic or epidemic acute disease, to an origin in chronic disease. In The Chronic Diseases he wrote:
“Psora is that oldest, most widespread, most destructive, and yet most misunderstood chronic miasmatic disease which for many millennia disfigured and tormented peoples, but in recent centuries has become the mother of all the thousands of incredibly diverse (acute and) chronic (non-venereal) ailments that now increasingly afflict civilized humankind throughout the inhabited earth.”
Specifically excluding the venereal chronic diseases from dependence on Psora, but appearing to implicate “all the thousands of incredibly diverse acute … ailments that now increasingly afflict civilized humankind throughout the inhabited earth.”
However, further on in the same text he wrote:
" It was easier for me than for many hundred others to discover and discern the signs of Psora, both those still slumbering and latent in the interior and those roused up out of the interior into serious chronic diseases, by careful comparison of the state of health of all affected with it with myself, because I, as is rarely the case, was never psoric, and hence, from my birth till now, when I am in my eightieth year, I have always remained completely exempt from all the ailments (great and small) described here and further on, though I am otherwise very susceptible to acute epidemic diseases, and although I have undergone much mental labor and thousands of emotional mortifications."
Clearly asserting that acute and epidemic disease is not necessarily predicated on Psora. Neither does he suggest that Syphilis or Sycosis need be predicated on Psora.
We certainly see some acute disease that is predicated on pre-existing chronic disease, as Hahnemann suggests in §73. Acute otitis media is often (¿always?) predicated on chronic disease, and often requires treatment of the underlying chronic disease to prevent recurrence. But this is not the norm; when measles is endemic in a community, 95% of non-immune children will acquire the disease before the age of 15, regardless of their chronic disease status. Falling off the roof while installing Christmas lights will result in a bruise in any of us (I’m picturing Clarke W. Griswold; now perhaps getting up there in the first place is another story).
The chronic miasms are not fundamentally states of susceptibility - they are chronic diseases - but they may create susceptibilities to particular morbid influences, resulting in the disposition to develop particular acute diseases. We might add to §73 in the Organon, specifying the category of acute exacerbations of chronic disease.
A singular ancestral acquired susceptibility to disease (in this case, a falling out of grace) fits in with Kent’s theological philosophy, but is inconsistent with Hahnemannian thought and with observation.
We’ll often encounter arguments e.g. that an ulcerating acute disease is “syphilitic” based on the assertion that ulceration & tissue destruction is fundamentally a property of Syphilis; or that acute diseases involving excess or proliferation - including mental/emotional “excesses” - are “sycotic.” There is no basis to this. Syphilis is certainly known for its chancres, but it does not hold the market on ulceration, which may be seen in many other diseases as well, both acute and chronic. A herpes infection is not syphilitic, sycotic, or psoric - it is herpetic.
Much of the current interest in “miasms” comes from Rajan Sankaran’s “schema” approach to prescribing; looking for an intersection between proposed “Kingdoms”/“families” themes and the themes of the 10 categories he’s presented as “miasms.” We might discuss the utility of this approach in another setting, but importantly, the categories advanced as “miasms” are not miasms or other natural categories, even if 3 of them bear the names of Hahnemann’s chronic miasms, and all save one bear the names of communicable diseases; but are categories humanly constructed for convenience, and might better be given another, more appropriate name. In any event, if they were in fact chronic miasms, they’d be applicable to chronic disease, but not to acute disease.
James Tyler Kent, 1900, Lectures on Homeopathic Philosophy, Lecture 18 http://www.homeoint.org/books3/kentlect/lect18.htm
Samuel Hahnemann, Organon of the Art of Healing, 6th edition
Samuel Hahnemann, 1828, The Chronic Diseaseshttp://www.homeoint.org/books/hahchrdi/index.htm
Wikipedia, Natural Kinds https://en.wikipedia.org/wiki/Natural_kind
Bio
Will Taylor (03/22/1951- ) graduated from the University of Vermont College of Medicine in 1979 and completed a residency in Family Practice at St. Mary’s hospital in Milwaukee, Wisconsin, initially practicing conventional family medicine in Bethel, Maine. An painful episode of shingles led him to seek the care of a colleague practicing homeopathy, and a single dose of Rhus tox 1M sent him on a journey into homeopathic medicine, first in treating his 2 sons, who caught chickenpox from his shingles outbreak, then, after pursuing formal study with the The International Foundation for Homeopathy, as an option for patients in his medical practice. In 1993, Will pulled the plug on conventional practice and opened a practice devoted to homeopathy in Blue Hill, Maine, moving in 2001 to Portland, Oregon to teach full time at the National College of Natural Medicine. Will has served as faculty at The School of Homeopathy New York, the Homeopathic Academy of Southern California, and the Czech Medical Homeopathic Association, and has shared his experiences in homeopathy at National & State Societies in the U.S., & in Austria, Germany, Bulgaria and Slovakia, and online since the early days of the internet. He is currently retired after a disabling stroke in 2014, living in a cabin in the Maine Woods on Mt. Desert Island. His current projects include maintaining an archive of online video courses at https://courses.homstudies.com/, writing a growing collection of articles & essays at https://willtaylormd.substack.com, and a growing collection of eBooks at https://payhip.com/homstudiescom.