A Scientific Approach to the Study and Practice of Homeopathy
By Vijay H. Vaishnav M.D. (Hom.), CCH
Homeopathy today resembles the allopathy of Hahnemann’s time. It has become both a medicine of experience and a medicine of theories.
It has now become fashionable to churn out new theories on homeopathy, and often the same homeopath introduces a new theory on a yearly basis. Another growing trend is to be a nonconformist - making highly peculiar prescriptions with equally peculiar remedies, so that all those attending the seminars and conferences look up to the speaker with awe and respect. While this may win the admiration of the audience, the unfortunate patient can become little more than a guinea pig! Perhaps Hahnemann foresaw what might happen 200 years later, as suggested by this passage from his Lesser Writings1:
“In order accurately to perceive what is to be observed in patients, we should direct all our thoughts upon the matter we have in hand, come out as it were, and attach ourselves, so to speak, with all our powers of concentration upon it, in order that nothing that is actually present, that has to do with the subject, and that can be ascertained by the senses, may escape us. Poetic fancy, fantastic wit and speculation must for a while be suspended, and all over-strained reasoning, forced interpretation and tendency to explain away things, must be suppressed. The duty of the observer is then only to take notice of the phenomena and their course; his attention should be on the watch, not only that nothing actually present should escape his observation, but that also what he observes be understood exactly as it is.”
Rational Prescribing
What are the pre-requisites to be rational in our approach to prescribing? The most important of course is history. A case well taken is half cured is an adage credited to the noted classical homeopath Elizabeth Wright Hubbard, and rightly so. Dr. Herbert A. Roberts emphasizes this: “The physician's degree of success in obtaining the proper symptom picture lies in his skill and patience. We cannot rush these patients through. We must be good listeners. Get the patient to talking, and tactfully keep him talking about the symptoms rather than wandering far afield. Then cultivate your powers of listening and give your powers of observation full sway, to form the complete picture of the little details and habits of your patient. It has been said that criminal lawyers should be medical men; it is eminently necessary, however, that homeopathic physicians be past masters of the art of cross-examination; and the observance of the patient's every movement and expression should be a matter of record.2”
Next, is to understand what is to be cured in disease, as mentioned in Aphorism 3 of the Organon3:
“If the physician clearly perceives what is to be cured in diseases, that is to say, in every individual case of disease (knowledge of disease, indication), if he clearly perceives what is curative in medicines, that is to say, in each individual medicine (knowledge of medical powers), and if he knows how to adapt, according to clearly defined principles, what is curative in medicines to what he has discovered to be undoubtedly morbid in the patient, so that the recovery must ensue – to adapt it, as well in respect to the suitability of the medicine most appropriate according to its mode of action to the case before him (choice of the remedy, the medicine indicated), as also in respect to the exact mode of preparation and quantity of it required (proper dose), and the proper period for repeating the dose; – if, finally, he knows the obstacles to recovery in each case and is aware how to remove them, so that the restoration may be permanent, then he understands how to treat judiciously and rationally, and he is a true practitioner of the healing art.”
In the chapter on ‘Homeopathy and the Fundamental Laws’ in The Principles and Art of Cure by Homeopathy4, Dr. Roberts writes: “Biology gives us this law: FUNCTION CREATES AND DEVELOPS THE ORGAN. It has been observed in the study of homeopathy that functional symptoms are produced by the vital force in exact proportion to the profundity of the disturbance. Often, however, when pathological changes occur the symptomatic picture changes greatly in that functional symptoms do not manifest themselves in as great a degree; the disease condition has struck deeper and manifests itself less on the surface. Following the biological law, therefore, homeopathy postulates the law of symptom development: FUNCTIONAL SYMPTOMS PRECEDE STRUCTURAL CHANGES.”
This means we must know the basic sciences thoroughly. That is why, during homeopathic training, students are taught Anatomy (normal structure) and Physiology (normal function), followed by Pathology (abnormal structure and function), and then the clinical subjects like Medicine (as well as Surgery and Gynecology in most homeopathy schools worldwide). Mastery of both the pre-clinical and clinical subjects is essential because it enables one to differentiate between the common and characteristic symptoms in each diseased state. It is equally important to integrate this knowledge with one’s knowledge of homeopathy.
The American Institute of Homeopathy defines a homeopathic physician as “one who adds to his knowledge of medicine a special knowledge of homeopathic therapeutics and observes the law of similars”5. This means that one must first be a good clinician in order to be a good homeopath. Clinical skill should be the primary foundation used when making a prescription.
The following examples illustrate how these basic subjects may be utilized by a homeopath in making sound prescriptions.
Anatomy, Physiology, and Remedy Differentiation
Anatomy: This also relates to the sphere of action (S/A) of a remedy. Boger6 emphasized the importance of location in prescribing, and this remains highly relevant today. Each drug in the Synoptic Key has the heading “Regions”. Without a clear understanding of each remedy’s sphere of action, accurate prescribing becomes difficult. When you combine the knowledge of a drug’s sphere of action and its pathogenesis with an understanding of the underlying pathology, you are more likely to prescribe successfully. This approach is especially valuable in mastering acute prescriptions. Consider the knee joint, for example:
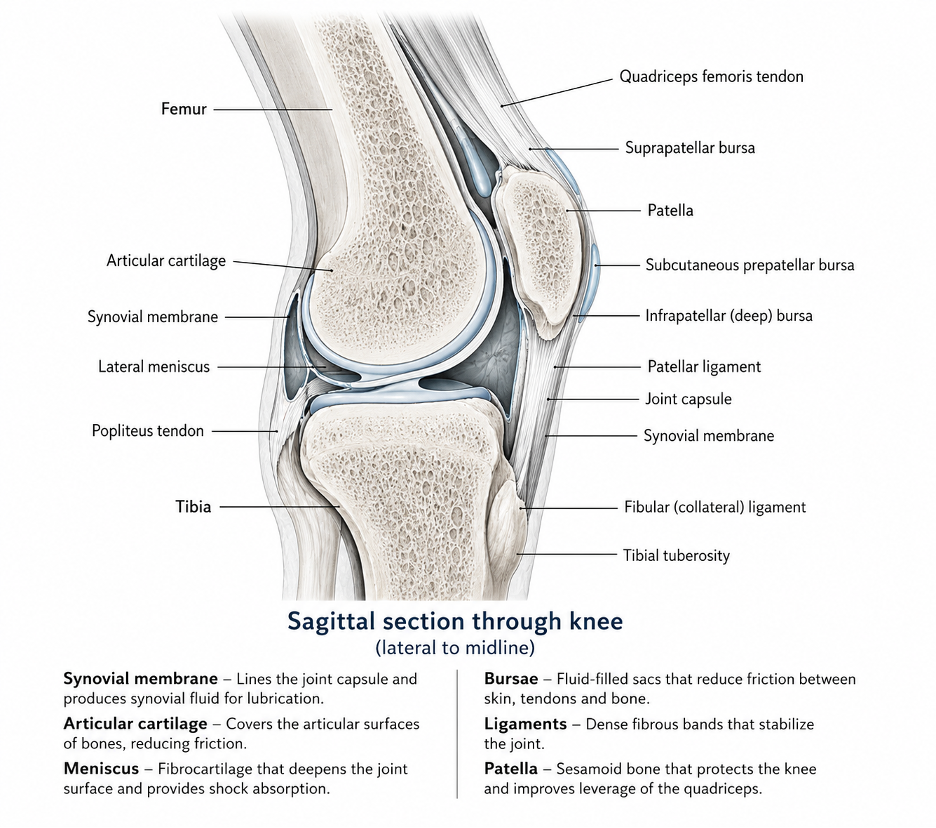
Sagittal section through knee, lateral to midline
The illustration above depicts a sagittal or longitudinal section of the knee joint. Each anatomical part of the joint will need a different homeopathic remedy even though the patient has “arthritis”.
A person who comes to you with an acute pain in the knee joint < rest, < initial motion, > continued motion will bring to your mind three important remedies- Rhus toxicodendron (Rhus tox), Ruta graveolens (Ruta) and Calcarea fluorica (Calc fluor) So how do we decide which of these remedies should be given for the acute symptoms? The anatomical part affected and the sphere of action of the drug will help.
If the white fibrous tissue and aponeurosis around the joint is the cause of the pain, Rhus tox is the remedy. If the cartilage, the meniscus or the cruciate ligament is affected with these modalities, the drug of choice would be Ruta. If the patient has an X-ray of the knee that shows osteophytes- signs of degenerative osteo-arthritis, we could consider Calc fluor for the same set of symptoms.
A person who has been diagnosed with acute synovitis or inflammation of the synovial membrane in the knee joint may need either Bryonia alba (Bryonia) or Apis mellifica and will rarely be prescribed Ruta or Calc flour for it.
When there is an inflammation of the outer layer of the bone or periostitis, homeopaths consider this an expression of the syphilitic miasm and, the remedies like Kali bichromicum, Kali iodatum, Aurum metallicum (Aurum), etc. may be considered.
When the cortex of the bone, either the femur, tibia or fibula is affected with sepsis and infection- osteomyelitis, then the remedies to be considered are Hepar sulphuris calcareum, Silicea, Aurum, Asafetida, Fluoricum acidum etc. (Hekla lava is also a good remedy for osteomyelitis, but the specific anatomical structure is the lower jaw.)
If the patient has been diagnosed with bursitis causing acute pain- we should consider the use of Sticta pulmonaria- especially for infra-patellar bursitis- William Boericke has these symptoms mentioned in the drug Sticta pulmonaris, “Spot of inflammation and redness over the affected joint. Housemaid’s knee”. (Housemaids often need to kneel to sweep or to wipe objects. That leads to an inflammation of the bursa just below the patella and can cause the symptoms we find in the drug Sticta Pulmonaris.)
Physiology: Let me highlight the importance of physiology in making a correct prescription with the simple example of a frequently used remedy.
We often use the remedy Arsenicum album (Arsenicum) in bronchial asthma. The most important modality that comes to our mind when we think of this remedy is the midnight aggravation. However, when you use this modality to prescribe Arsenicum in asthma, you often find that you do not get the desired response, and the patient seems to be getting worse even though you used the keynote modality of Arsenicum -. Many of my students have come to me with this question- “Why didn't the Arsenicum work when I used the peculiar general time modality as the basis of my prescription?” And I tell them- you have picked a common symptom.
Serum cortisol levels in the human body are at their lowest at around midnight. As is well known, cortisol helps keep the immune response in check,and in conventional medicine the treatment of severe acute attacks of bronchial asthma are often treated with cortisone in tablet or injectable form. So, the organism has the least protection against allergens at around midnight and is most likely to get an attack of asthma.
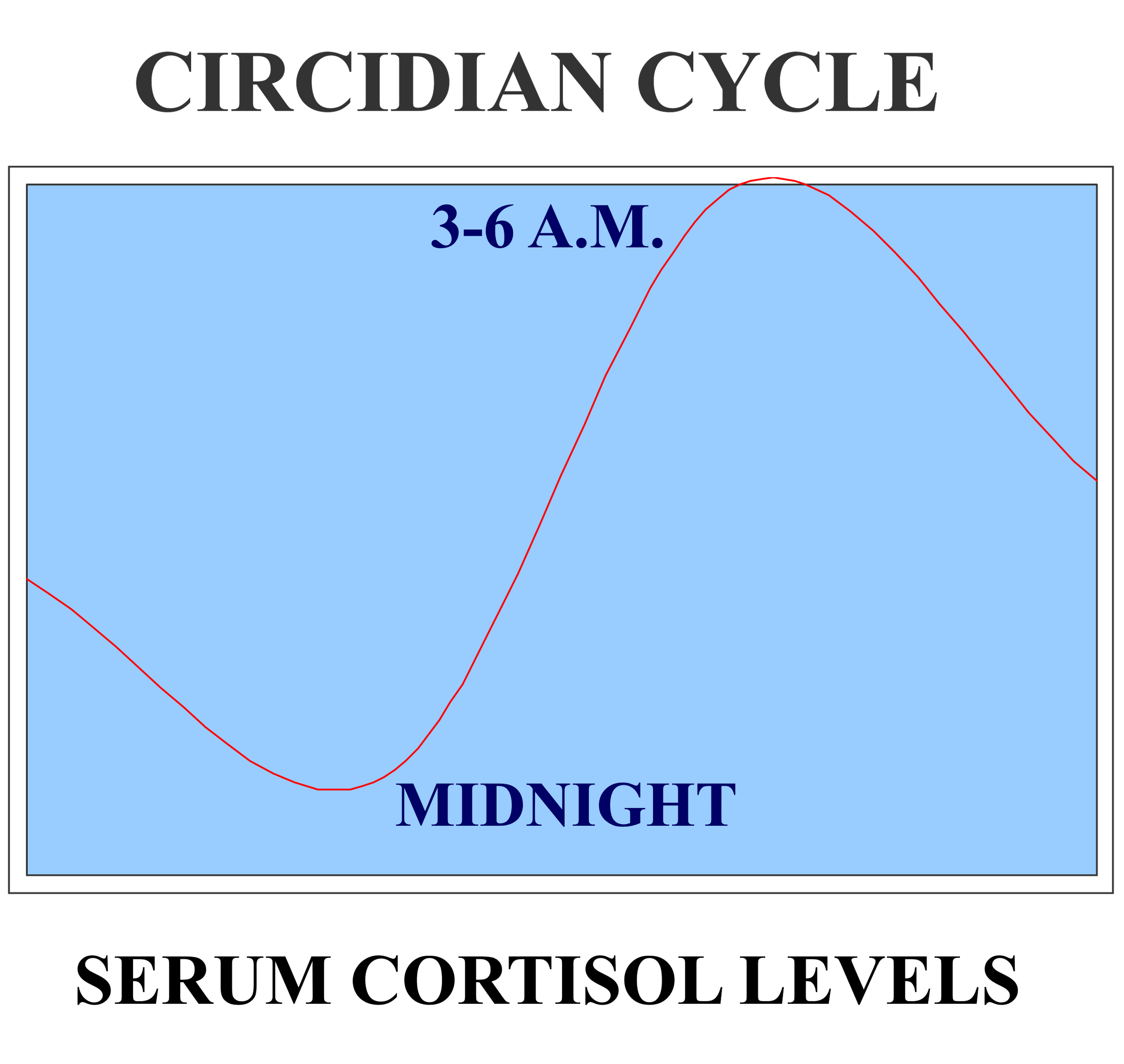
Circadian Cycle of Serum cortisol
At about 4 am, the Serum Cortisol levels are at their peak, and if at this time of the day a patient gets an attack of asthma, I would consider it to be more important and characteristic. Hence the < 3 or 4 am of Kali carbonicum, Nux vomica (Nux v), Ammonium carbonicum, Antimonium tartaricum, Thuja occidentalis (Thuja) is a characteristic symptom of bronchial asthma.
I have a very strong suspicion that James Tyler Kent also faced this in his practice! In his Lectures on Homeopathic Materia Medica in the chapter on Thuja, he writes “A peculiar asthmatic condition is found in sycosis and Arsenic appears to be indicated for the symptoms, but it only relieves, it does not control the predisposition, it acts like Aconite in acute diseases and only ameliorates for a moment. Asthmatic and many other sycotic conditions seem to call for Arsenic, but it will do nothing but palliate, the constitutionality is not reached by Arsenic, its fundamental symptoms are not similar. In syphilis and psora Arsenic acts a long time and eradicates the complaints, when similar to them, but it is not similar to sycosis. Arsenic does not go to the bottom of the trouble, but Thuja and Natrum sulph. will take up the work and cure. Natrum sulph. and Thuja bring back the primitive manifestation that has been suppressed for years.”
I believe the knowledge of physiology was not advanced during Kent’s time as it is now and so he tried to explain this with the concept of miasm. But, if you notice, he mentions that the drugs Thuja and Natrum sulphuricum (Nat sulph) will cure if Arsenicum fails, and these drugs have < 3 am or < 4-5 am respectively. This fits with our knowledge of the circadian cycle of cortisol in the human body.
Pathology and Remedy Differentiation
Pathology: Is it essential to keep the underlying pathology in mind? Do we need to correlate the pathology in the patient and the pathogenesis of the drug when we prescribe?
The knowledge of pathology helps us decide the miasm, the susceptibility of the Vital Force, the selection of the potency and repetition of the remedy. It also helps us in selecting the homeopathic remedy and differentiating between remedies. I think a few examples from the Materia Medica will make the answer obvious.
We have three important remedies for constipation from inactivity (i.e. no desire for stools)- Bryonia, Alumina and Opium. All three have apparently the same symptom, yet they are different.
Bryonia has inactivity from dryness. This, of course, is a leading indication of the drug. The stools are large, dry, hard, blackish as if burnt, with no desire to have a bowel movement for several days.
Alumina’s constipation arises from paralysis. The paralysis affects the muscles of the rectum. Hence, even a soft stool requires great straining.
Opium has paralysis too. But it is of the whole alimentary tract, and the patient develops obstinate constipation with no desire to pass stool. The stools are hard, round, black balls.
On the other hand, we have three important drugs for constipation with an ineffectual urge to pass stools- Nux vomica (Nux v), Carbo vegetabilis (Carbo veg), and Lycopodium. Once again, the underlying location and pathology will differentiate the drugs.
The ineffectual urge for stools in Nux v is due to an irregular peristaltic activity of the intestines. By the time the Nux vomica patient reaches the toilet, this irregular peristaltic wave has gone, and they do not pass much stools. (It is not reverse peristalsis- that would cause fecal vomiting as in Plumbum metallicum.)
Carbo veg has flatulence as its guiding symptom. It is this flatulence that causes this urging for stools in this drug. The rectum gets distended with flatus and stretches the stretch receptors there. These receptors send a signal to the brain (incorrectly) that the rectum is filled with fecal matter, and they get the urge to pass a stool. However, when they do use the toilet, all that is passed is gas and the urge diminishes and there is relief. As we know, > flatus is also an important modality of Carbo veg.
Lycopodium has this same symptom due to a spasm of the anal sphincter. This could be due to a condition called proctalgia fugax. The mental state of Lycopodium fits perfectly with the patient profile- anxious personality, professionals like lawyers, accountants who are under tremendous stress and have anticipatory anxiety, etc. The anal spasm causes the Lycopodium patient to get this ineffectual urge for stool.
Sometimes, two drugs have similar symptoms where location, sensation and even modalities might be similar. Under such circumstances, knowledge of the underlying pathology is useful.
An example is seen in the head section excerpted from a drug found in Boericke’s Pocket Manual of the Materia Medica.
“As if skull would burst. Sensation as if the brain were balancing to and fro, and striking against skull, receiving great pain. Intense throbbing of head and carotids. Spasmodic headache in vertex, with subsequent pain, as if bruised in sides of head. Face flushed. Relieved from pressure and warm room. Scalp sensitive; worse combing hair. Aches worse in open air, from temple to temple. Worse by contact, current of air, stepping.”
I am sure most of you read these symptoms and concluded that the remedy is Belladonna. However, you will be surprised to know that these are actually the head symptoms of China officinalis (China) (from the Cinchona officinalis species) in Boericke7. There is one symptom that I had purposely left out in the quote above “Face flushed after hemorrhages, or sexual excesses, or loss of vital fluids.” This is the underlying pathology in China- loss of blood causing anemia.
It is therefore easy to differentiate two drugs with similar symptoms if you know the underlying pathology. Belladonna has the same symptoms when there is actual inflammation, whereas China has these symptoms from anemia.
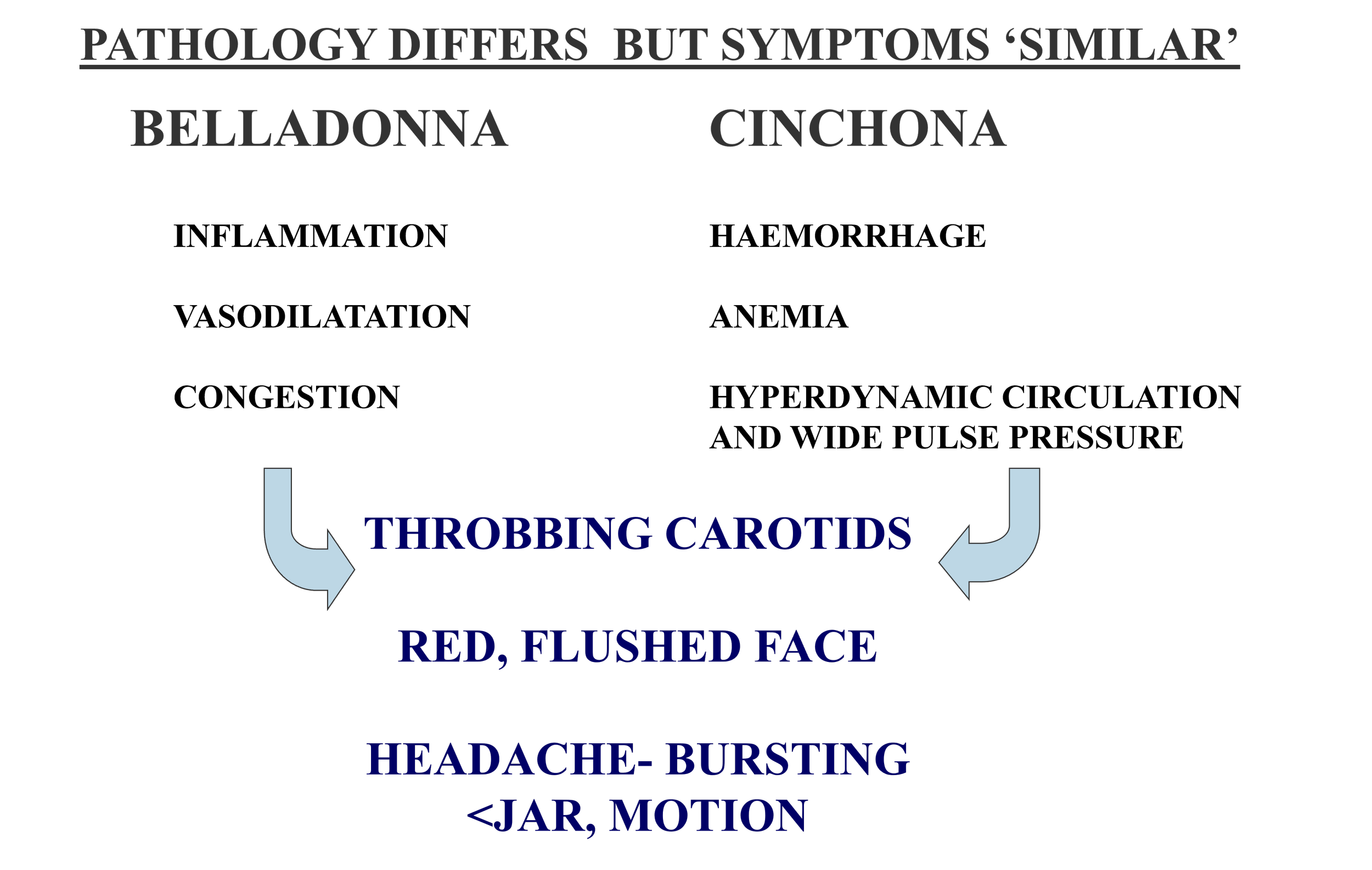
Belladonna comparison with Cinchona, underlying pathology for headache with bursting pain worse from motion symptom
So, the next time a patient presents with a similar headache, examine them carefully. Could anemia be underlying the case - and therefore indicate China?
Talking of anemias, another drug that comes to my mind is Alumina. All the leading indications point towards its possible use in anemia, but if you study them closely, you will find symptoms of Iron deficiency as well as Vitamin B12 deficiency, i.e. dimorphic anemia. The chart below classifies the symptoms of Alumina from Boericke8 into the general symptoms of anemia as well as the symptoms of Iron deficiency and Vitamin B12 deficiency. It needs to be underscored however, that Alumina is not a substitute for iron and Vitamin B12 supplements. When Alumina is prescribed as a constitutional remedy, it will help in the absorption and assimilation of these substances from the diet.
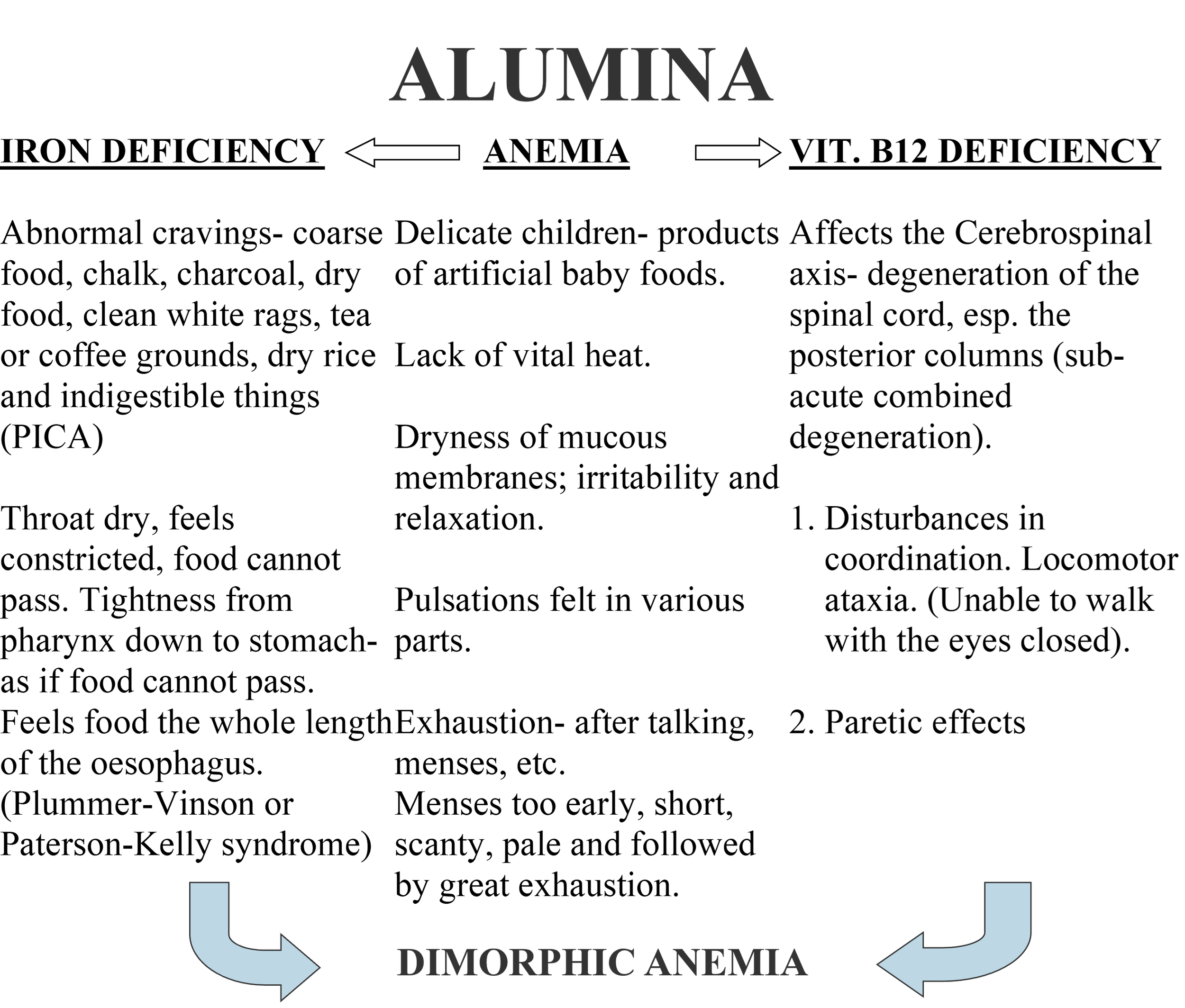
Alumina remedy symptoms of underlying dimorphic anemia
The Study of the Materia Medica
At this point I wish to highlight how the Materia Medica should be studied in order to understand the guiding symptoms of the remedy. The keyword is understanding the symptoms and not learning them by rote. To do this, I teach my students the importance of the role of Sphere of Action (S/A) and Pathogenesis of the drug and how they lead us to the guiding symptoms.
Let us take Pulsatilla as an example. Its important guiding symptoms are Chilliness (more the pain, more the chilliness), < Evening, < Warm room, > Open air, > Slow, gentle motion. The pictorial representation below explains how knowledge of the drug’s sphere of action and pathogenesis helps explain its guiding symptoms:
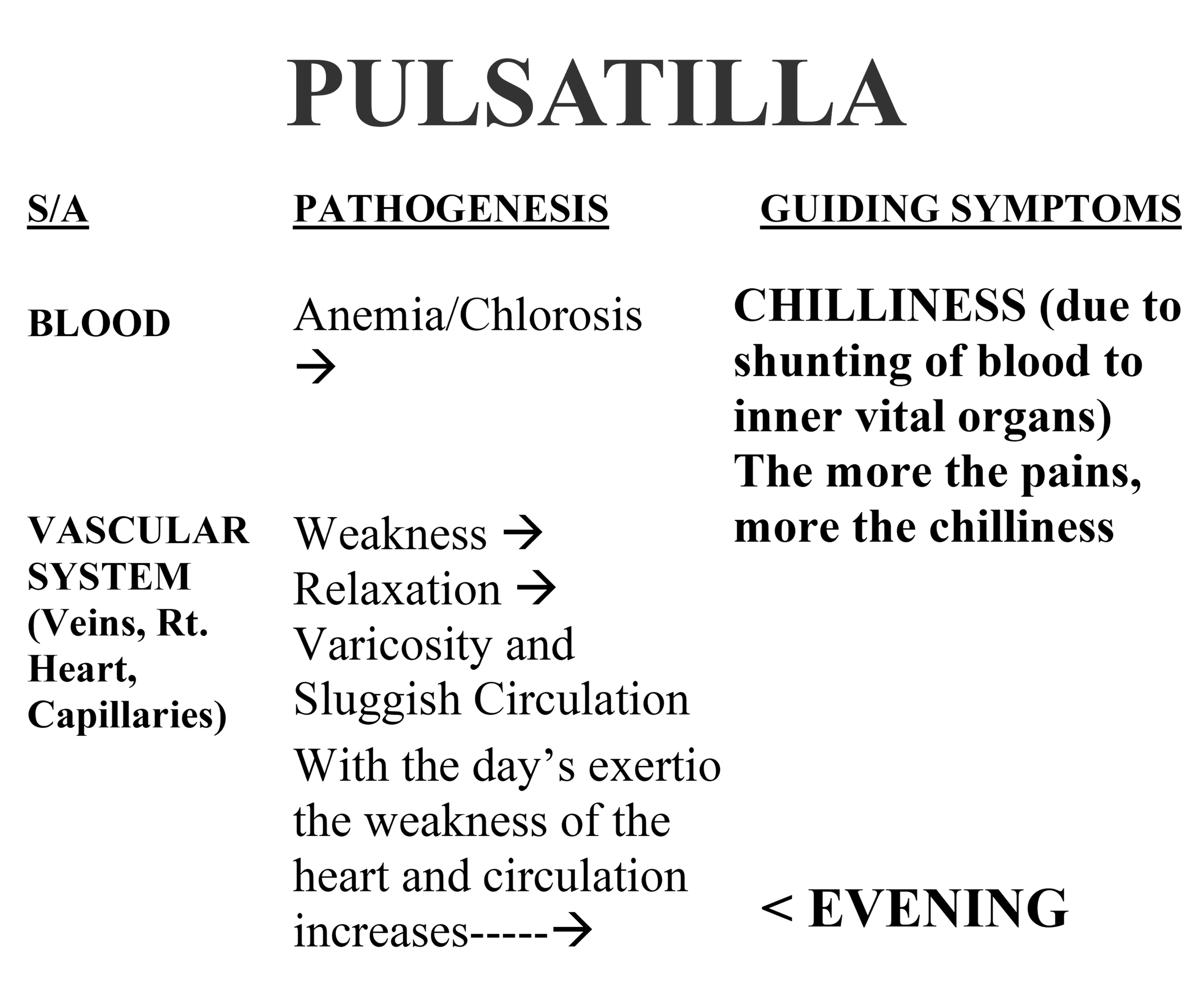
Pulsatilla underlying anemia and sluggish circulation resulting in Chilliness in evening
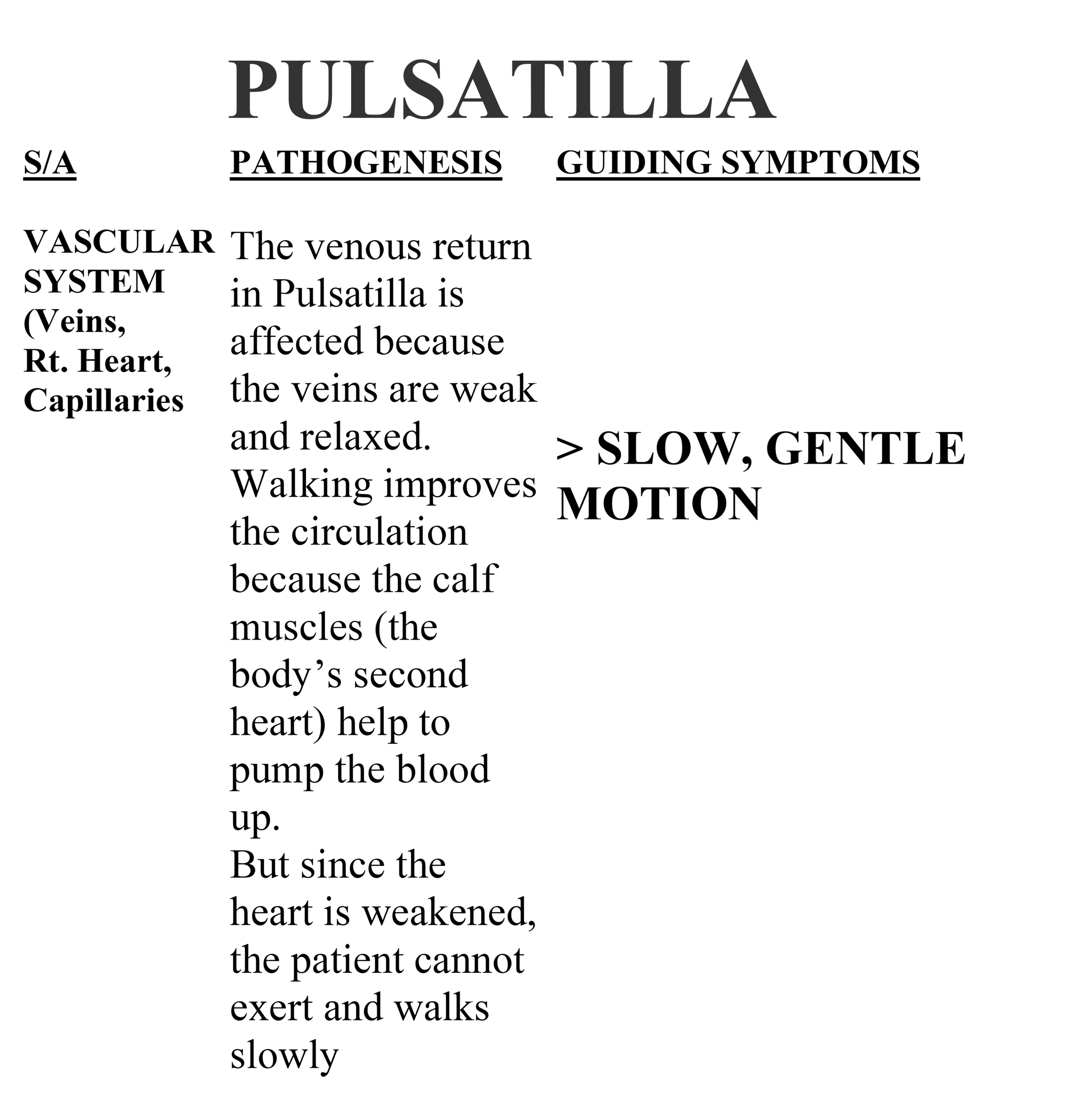
Pulsatilla better slow gentle motion symptom underlying physiology
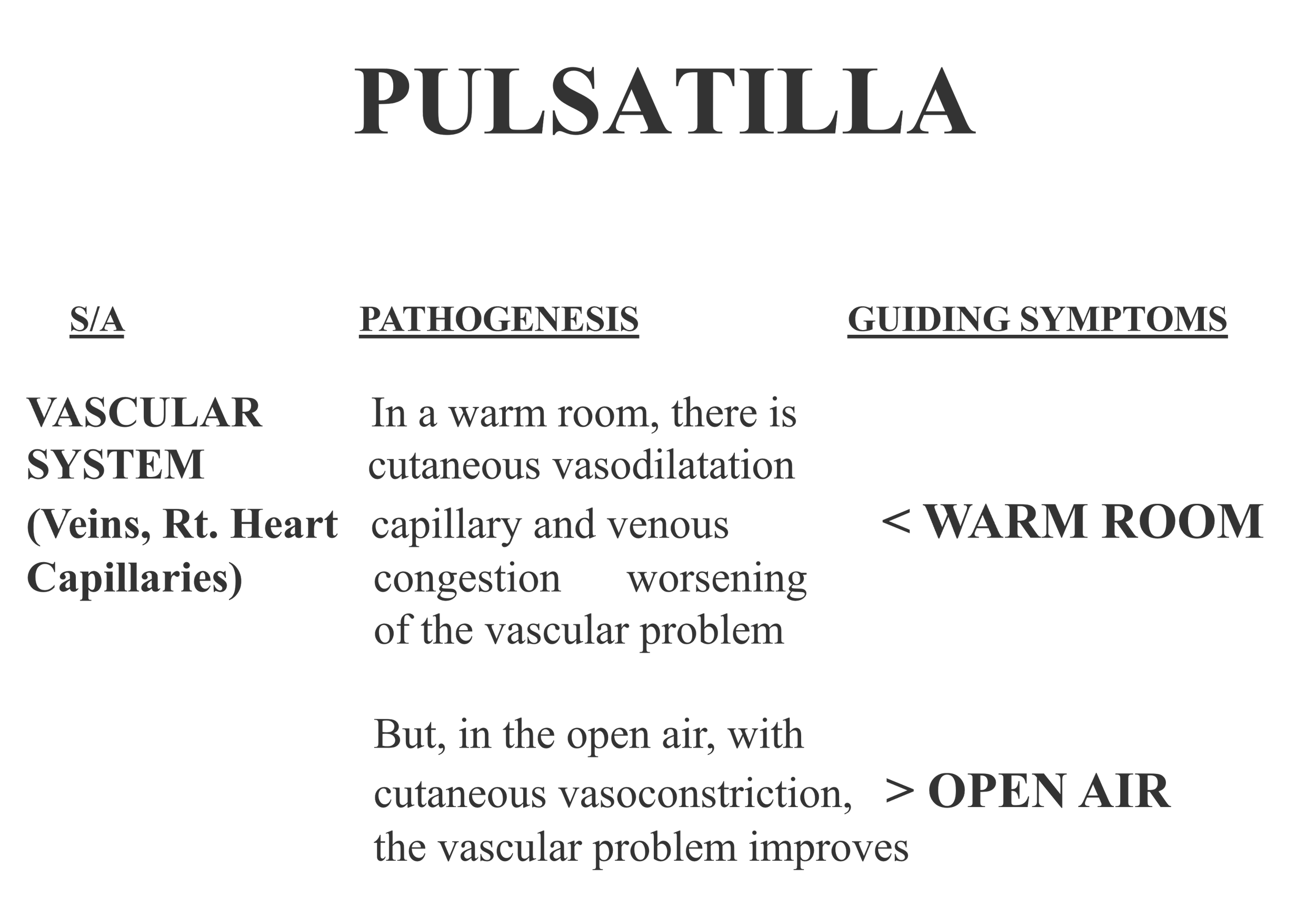
Pulsatilla improved vasculature in open air, vasodilation in a warm room
Case Studies:Practical use in homeopathic prescriptions
The following two case examples illustrate the use of the knowledge of anatomy, pathology and clinical medicine to prescribe for patients who have gross pathological conditions. These cases were under my care at the teaching hospital attached to our homeopathic college in Mumbai, India (where I taught Homeopathic Materia Medica and Medicine for about 25 years before setting up practice in the USA). While I was teaching at the college, we had developed an integrative approach wherein a physician from the conventional medicine system and a homeopath would see the patients together in the Out Patient Clinics and then decide what would be the best treatment suited for the patient. In most instances, the physician had a diagnostic and supportive role, and the homeopath would prescribe the indicated remedy.
The cases described below were prescribed the so-called “rare remedies”. I have used the term ‘so-called’ because I do not believe that a remedy that is part of any book of Materia Medica is rare. It has been proved on healthy human volunteers and only after that does it make it to the Materia Medica (or the pharmacopeia). There is NO rare remedy. It is called rare by some, mainly because they have not heard of it or studied it or used it in practice.
Case 1:
A 63 years old farmer was admitted with the chief complaint of progressing dyspnea. The diagnosis was Congestive Heart Failure. Breathlessness < lying down, warm room > open air
He felt the heart beating all over the chest.
On further interrogation:
The bladder feels full, with frequent urge to urinate, urine is scanty and offensive.
No general symptoms elicited.
Only two mental symptoms elicited:
Dullness of the mind; cannot think properly (this symptom was given by his son)
Irritability, especially when asked any question.
On examination: all the signs of gross cardiac failure were present including edema feet and puffiness of the face.
EKG: T wave- inverted tick mark (indicating Digitalis toxicity)
2D Echocardiogram (Ultrasound of the heart): Dilated cardiomyopathy
This diagnosis indicates a poor prognosis. Paucity of symptoms + advanced pathology made us think of a drug covering the heart pathology, and we decided to give in a low potency with frequent repetitions.
Treatment: Convallaria majalis was the drug selected (when the ventricles are over distended and dilatation begins and there is an absence of compensatory hypertrophy and when stasis is marked9).
15 drops of the Φ (this is the symbol traditionally used to denote the mother tincture in India) diluted in 30 ml of water were given every 3 hours and simultaneously the dose of Digoxin was reduced.
Result: Within 12 hours, the urinary output increased and by the 3rd day, we had drained him of his excess fluids. His edema disappeared and he was no longer dyspneic.
Case 2:
A 70 years old male patient, with a 40 year history of Chronic Bronchitis was admitted with an acute exacerbation. When I visited him in the wards, he was quite breathless with a lot of mucus rattling in his chest. Expectoration was extremely difficult.
He was already on bronchodilators, antibiotics, expectorants, and nebulization as well as respiratory physical therapy without any relief.
On examination: B.P.- 174/82 mm. Hg;
Respiratory System- occasional rhonchi, crepitations/rales ++
X ray chest: Broncho vascular markings ++
EKG: P –pulmonale (tall, peaked P-waves indication a Right atrial enlargement)
Treatment: Baryta muriatica (Bartya mur) 30c, dry on the tongue, three times a day
Result: The patient started expectorating freely and was relieved of his dyspnea. His respiratory signs disappeared within 4 days.
Discussion:
The patient was not in a condition to give his symptoms nor was he willing to do so. We had to rely only on the examination and investigation findings. Baryta mur is an important remedy for ‘bronchial affections of old people with cardiac dilatation. It facilitates expectoration. Great accumulation and rattling of mucus with difficult expectoration. Arteriosclerosis of the lungs, thus in senile asthma, modifies the arterial tension’10. (Arteriosclerosis of the lungs, as mentioned in the homeopathic literature, could clinically point to Pulmonary Hypertension.)
Organ remedies, or locally acting remedies, are often needed in some incurable cases where palliation forms the main treatment plan. A deep acting remedy given to a patient with gross organic changes or when the Vital Force has lost its power to react, i.e. when susceptibility is low, may cause severe aggravations as mentioned by Kent11.
Conclusion
Homeopathic prescribing is therefore not solely on mental symptoms, dreams, or physical symptoms alone. A prescription should be a blend of both the mental and physical aspects of the case. The constitutional remedy is what one should always seek when formulating a classical homeopathic prescription. However, one must also consider the underlying pathology to make the correct diagnosis of the underlying miasm, and the appropriate remedy for that patient.
An integration of knowledge from the pre-clinical, para-clinical and clinical sciences is essential for the proper study of the remedies within our Medica Medica and for making rational and accurate prescriptions.
References:
Dudgeon R. E., (First Edition), The Lesser Writings of Samuel Hahnemann, B. Jain Publishers, (The Medical Observer, pages 724, 725)
Roberts Herbert A., Reprint edition 1981, The Principles and Art of Cure by Homeopathy, B. Jain Publishers, (page 79)
Samuel Hahnemann, 6th Edition, (reprint 1980), Organon of Medicine, B. Jain Publishers, (pages 92, 93)
Roberts Herbert A., Reprint edition 1981, The Principles and Art of Cure by Homeopathy, B. Jain Publishers, (page 59)
Farrington Harvey, Reprint edition 1994, Homeopathy and Homeopathic Prescribing, B. Jain Publishers, (page 1)
Boger C. M., (1931, Reprinted 1984) A Synoptic Key of the Materia Medica, B. Jain Publishers
Boericke, William, (1927, reprinted 1984), Pocket Manual of Homeopathic Materia Medica, (9th edition), B. J. Publishers, (pages 207, 208)
Boericke, William, (1927, reprinted 1984), Pocket Manual of Homeopathic Materia Medica, (9th edition), B. J. Publishers, (pages 34, 35)
Boericke, William, (1927, reprinted 1984), Pocket Manual of Homeopathic Materia Medica, (9th edition), B. J. Publishers, (pages 232, 233)
Boericke, William, (1927, reprinted 1984), Pocket Manual of Homeopathic Materia Medica, (9th edition), B. J. Publishers, (page 110)
Kent, James Tyler, (1900, reprinted 1981), Lectures on Homeopathic Philosophy, B. J. Publishers, (pages 253-265, 274-276)
About the author
Vijay Vaishnav, MD (Hom.), CCH
A former full-time Professor and Chair of Homeopathic Materia Medica at CMP Homeopathic College, Mumbai, Vijay has over 40 years of clinical and teaching experience worldwide. His private practice, honed by intensive Internal Medicine training at KEM Hospital, Mumbai in India, includes allergies, asthma, arthritis, children’s diseases, kidney and eye conditions,
He has been a subject matter expert for the Central Council for Research in Homeopathy of the Government of India, reviewing and contributing to their publications. Vijay has also taught in the USA at the American Medical College of Homeopathy, Arizona, the National College of Naturopathic Medicine, Oregon, and the Caduceus Institute of Classical Homeopathy, California. He is on the Board of the California Homeopathic Medical Society, the Editorial team of The California Homeopath and the Editorial Advisory Board of the Journal of Integrated Standardized Homeopathy, with numerous publications to his name.
He is currently practicing Classical Homeopathy in the Bay Area of California, USA.
More about him at https://drvaishnav.com